Previous introductory blogpost to this series.
Preamble: Random thoughts on spas
Part 1: Dual nature of touch: as PTs, do we "get" this? Part 1a: Touch can be pleasant, rilling Part 1b: Vallbo on C-tactiles
Part 2a: Different kinds of touch
...................
Next part of Skin as a Social Organ re: touch in affiliative behaviour and communication:
"What is the role of ‘‘pleasantness’’—the positive hedonic facet—in these categories of human social touch? First, pleasant touch may serve as a foundation for affiliative behavior. Second, it may provide a mechanism for the formation and maintenance of social bonds. Third, it is a nonverbal means for the communication of emotions. It is important to note that the above varieties of social touch are not always welcome or even pleasant; touch has an intricate relationship with culture, context, and gender (e.g., Dibiase and Gunnoe 2004), and, depending on these factors, pleasure easily tips into aversion and disgust."
Dibiase R, Gunnoe J (2004) Gender and culture differences in touching behavior. J Soc Psychol 144:49–62
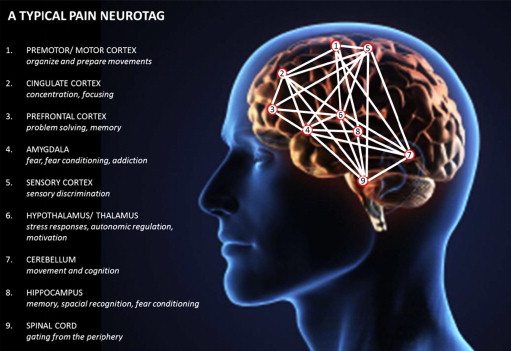
Oh yes, yes it can - pleasure from touch can tip easily into aversion and disgust. Easily. Aversion, disgust, and withdrawal from nociception are all processed by the insular cortex and anterior cingulate cortex.
As therapists who can touch people, we enjoy extended social trust from our patients that overrides their aversion, maybe disgust.. i.e., from being touched by a stranger. They also deliberately inhibit the urge to withdraw from nociceptive discomfort. Maybe too easily.
We really should take care to not add any nociception to an already overloaded nervous system if we can possibly help it. All it does is make nervous systems tense up unconsciously in some other part of the motor output system.
If we think of pain output as the patient's critter brain all freaked out about something, and it biting down hard on the patient from the inside, then it's easy to see why: Why hurt a distraught horse? be Monty Roberts instead - speak it's language, non-verbally: Why hurt a frightened snarling dog? Be Caesar Milano instead. Be the alpha dog, but be kind - outstare it instead.
As therapists who can touch people, we enjoy extended social trust from our patients that overrides their aversion, maybe disgust.. i.e., from being touched by a stranger. They also deliberately inhibit the urge to withdraw from nociceptive discomfort. Maybe too easily.
We really should take care to not add any nociception to an already overloaded nervous system if we can possibly help it. All it does is make nervous systems tense up unconsciously in some other part of the motor output system.
If we think of pain output as the patient's critter brain all freaked out about something, and it biting down hard on the patient from the inside, then it's easy to see why: Why hurt a distraught horse? be Monty Roberts instead - speak it's language, non-verbally: Why hurt a frightened snarling dog? Be Caesar Milano instead. Be the alpha dog, but be kind - outstare it instead.
........
The paper cited is a nice fat 15 page paper that looks carefully at power differential, status, culture, gender. It looks at touch as a means of communicating dominance in all these things, to others. I didn't see anything in it while reading through it about aversion or disgust, though, just a cataloguing of findings in general from other researchers and more about three cultures more specifically. Nothing one doesn't already know from general reading..
"Proxemics" factor in big time. Apparently, people from cold climate cultures prefer relatively larger physical distances when they communicate. People in cultures in warmer climates cozy up more.
I have noticed this personally visiting Mexico, Central American countries, Brazil. Lots more physical contact. Not at all unpleasant, just different. Unless you happen to be allergic to perfume, as I am.
A recent tidbit on this: if you have anxiety trait, you need more peripersonal space. Size of Personal Space Is Affected by Anxiety. Giandomenico Iannetti and Chiara Sambo. Better safe than sorry? The safety margin surrounding the body is increased by anxiety. The Journal of Neuroscience, 2013
The defensive peripersonal space represents a “safety margin” advantageous for survival. Its spatial extension and the possible relationship with personality traits have never been investigated. Here, in a population of 15 healthy human participants, we show that the defensive peripersonal space has a sharp boundary, located between 20 and 40 cm from the face, and that within such space there is a thin, “highest-risk area” closest to the face (i.e., an “ultra-near” defensive space). Single-subject analysis revealed clear interindividual differences in the extension of such peripersonal space. These differences are positively related to individual variability in trait anxiety. These findings point to the potential for measuring a range of defensive behaviors in relation to individual levels of anxiety. Such measures will allow developing procedures to test risk assessment abilities, particularly in professions that require reacting quickly to aversive stimuli near the body, such as firemen, policemen, and military officers. This may also lead to possible interventions to improve their performance under pressure.
I could have told them that... seems like a no-brainer.















{kind=link}
{kind=link}
{kind=link}